Last updated on Jun 2, 2026
DoL OWCP-915 2007-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
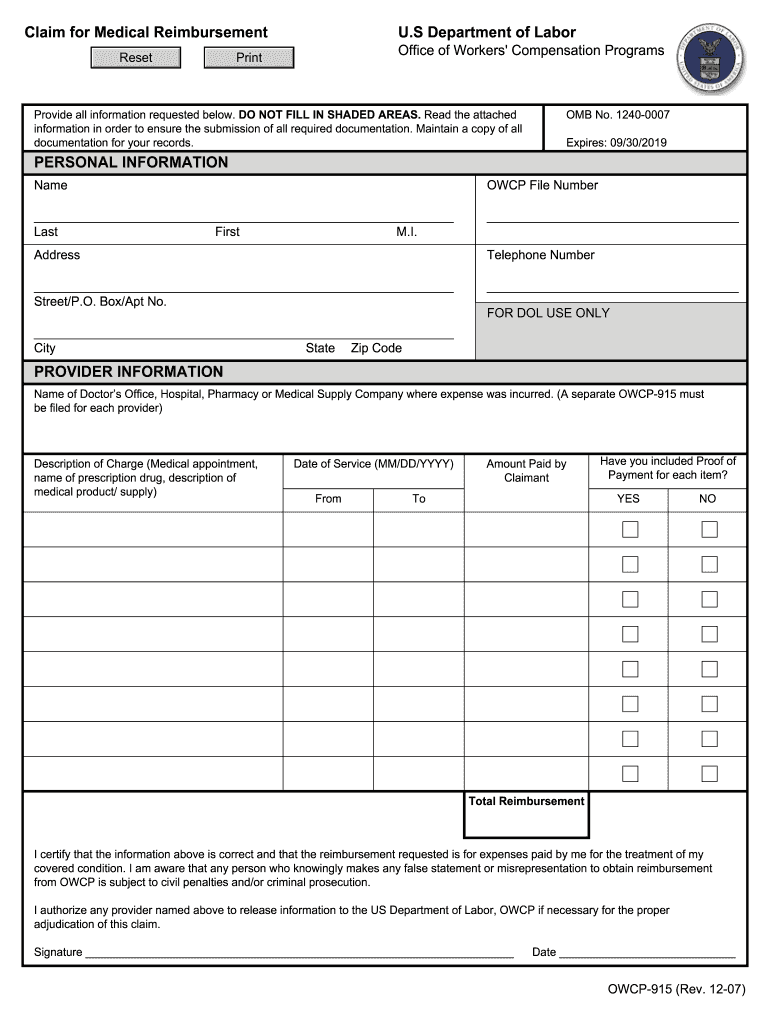
What is DoL OWCP-915
The US Department of Labor Medical Reimbursement Form is a government document used by claimants to seek reimbursement for out-of-pocket medical expenses related to accepted conditions under workers' compensation.
pdfFiller scores top ratings on review platforms
Very easy to use. Makes it simple and quick!
Great layout and easy to use, also helpful staff.
Who needs DoL OWCP-915?
Explore how professionals across industries use pdfFiller.

DoL OWCP-915 is needed by:
-
Employees injured on the job seeking medical expense reimbursement
-
Workers' compensation claimants requiring expense documentation
-
Healthcare providers submitting claims for services rendered to claimants
-
Legal representatives assisting clients with reimbursement claims
-
Government agencies overseeing workers' compensation processes
Comprehensive Guide to DoL OWCP-915
What is the US Department of Labor Medical Reimbursement Form?
The OWCP-915 form, known as the US Department of Labor medical reimbursement form, is critical for individuals seeking to claim medical reimbursements associated with workers' compensation. It serves as a formal request for reimbursement of out-of-pocket medical expenses incurred while treating conditions deemed acceptable by the Department of Labor.
This form becomes applicable under specific conditions, such as when a claimant has paid for necessary medical services related to a work-related injury or condition. Timely filing of this form is vital to ensure that claims are considered promptly and effectively.
Purpose and Benefits of the US Department of Labor Medical Reimbursement Form
The primary purpose of the OWCP-915 form is to empower claimants to recover out-of-pocket medical expenses. By utilizing this medical expense reimbursement form accurately, users can maximize their reimbursements and ensure that all eligible costs are considered.
Maintaining detailed records and comprehensive supporting documentation is essential. These practices facilitate a smoother claims process and contribute to a higher approval rate of reimbursement requests.
Who Needs the US Department of Labor Medical Reimbursement Form?
The OWCP-915 form is designed for individuals who have incurred medical expenses due to work-related injuries or conditions. Eligible claimants typically include employees covered under workers' compensation programs.
Failure to file this form or delays in the submission process can lead to significant consequences, such as denied claims and out-of-pocket costs that may become unrecoverable.
How to Fill Out the US Department of Labor Medical Reimbursement Form Online
Completing the OWCP-915 form accurately requires attention to detail. Start by filling out all claimant details, followed by providing accurate information about your medical provider.
Here are some tips for ensuring accuracy:
-
Double-check personal information before submitting.
-
Avoid common mistakes like omitting required fields.
Utilizing pdfFiller as a tool can streamline the process of filling out the form online effectively.
Required Documents and Supporting Materials
Before submitting the OWCP-915 form, it is crucial to gather necessary documents that support your reimbursement claim. Key documents include:
-
Receipts for medical treatments and services.
-
Invoices from medical providers confirming the costs incurred.
These documents are critical for the approval process, ensuring that your claim is backed by adequate evidence. Organizing your documents efficiently can help streamline the submission process.
Submission Methods for the US Department of Labor Medical Reimbursement Form
Once the OWCP-915 form is completed, it can be submitted through various methods. Online submission options provide a convenient route for many users.
If you choose to submit via mail, you'll need to follow specific instructions to ensure your form reaches the appropriate department. Additionally, keep in mind how to track the status of your submission after sending it.
Next Steps After Submitting the US Department of Labor Medical Reimbursement Form
After submitting the OWCP-915 form, claimants should be aware of the typical processing times associated with their claims. You can track the status to stay informed about your reimbursement request.
In the event of a claim rejection, it is vital to understand the next steps, including appeal options. Always keep copies of the submitted form and all supporting documentation to reference if needed.
Security and Compliance with the US Department of Labor Medical Reimbursement Form
Filling out and submitting the OWCP-915 form through pdfFiller ensures that your sensitive information is protected. The platform employs 256-bit encryption and complies with HIPAA and GDPR regulations to safeguard user data.
To enhance the security of your submission process, it is important to follow best practices for safeguarding personal and medical information at all stages.
Get Started with pdfFiller for the US Department of Labor Medical Reimbursement Form
Utilizing pdfFiller for completing the OWCP-915 form offers a streamlined experience. The platform provides easy tools for editing, filling out forms, and even digital signing options.
Start using pdfFiller today to enhance your form-filling efficiency for all your documentation needs.
How to fill out the DoL OWCP-915
-
1.Access and open the US Department of Labor Medical Reimbursement Form on pdfFiller by searching for it in the platform's template library or uploading it directly from your device.
-
2.Navigate through the form's interface, using pdfFiller's interactive fillable fields to input personal information, such as your name, address, and details regarding your medical condition.
-
3.Gather all necessary information before starting, including medical provider details, descriptions of services rendered, related expenses, and proof of payment such as receipts or invoices.
-
4.Complete each blank field thoroughly, ensuring accuracy in the reported expenses and attaching any required documents using the upload features within pdfFiller.
-
5.Review the completed form for any errors or missing information, and ensure you have signed where indicated to validate your submission.
-
6.Finalize your submission by saving your form within the pdfFiller account. You can choose to download a copy for your records.
-
7.Submit the form electronically through pdfFiller by selecting the submission option or follow the provided instructions for mailing, if applicable.

Who is eligible to use the US Department of Labor Medical Reimbursement Form?
Any employee who has incurred out-of-pocket medical expenses related to an accepted workers' compensation claim can use this form to seek reimbursement.
What documents must be submitted with this form?
You need to attach proof of payment, such as medical bills, receipts, and any other documentation that supports your claimed medical expenses when submitting the form.
How do I submit the completed US Department of Labor Medical Reimbursement Form?
The completed form can be submitted electronically via pdfFiller or printed and mailed to the appropriate department indicated in the form instructions.
Are there deadlines for submitting this form?
It’s important to submit your reimbursement claim as soon as possible. Failure to do so within the designated timeframe may result in denial of your reimbursement request.
What should I do if I make a mistake on the form?
If you realize there’s an error after submission, you should contact the processing authority immediately to understand how to rectify the mistake.
How long does processing take after submission?
Processing times can vary, but it usually takes several weeks for your claim to be reviewed and a decision to be made. Always check with the relevant department for specific timeframes.
Do I need to notarize the US Department of Labor Medical Reimbursement Form?
No, notarization is not required for the US Department of Labor Medical Reimbursement Form. However, your signature on the form must be present to validate your claim.
Related Content
Related Forms






Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.