Last updated on Mar 23, 2026
CMS-L564 S plantilla gratuita para imprimir
pdfFiller no está afiliado a ninguna organización gubernamental

Rellenar
Complete el formulario en línea con un sencillo editor de arrastrar y soltar.

Firmar electrónicamente
Agregue su firma legalmente vinculante o envíe el formulario para su firma.

Compartir
Comparta el formulario mediante un enlace y permita que cualquiera lo complete desde cualquier dispositivo.

Exportar
Descargue, imprima, envíe por correo electrónico o mueva el formulario a su almacenamiento en la nube.
Por qué pdfFiller es la mejor herramienta para sus documentos y formularios
Gestión documental de principio a fin
Desde la edición y la firma hasta la colaboración y el seguimiento, pdfFiller tiene todo lo que necesita para completar sus documentos de forma rápida y eficiente.
Accesible desde cualquier lugar
pdfFiller es totalmente basado en la nube. Esto significa que puede editar, firmar y compartir documentos desde cualquier lugar usando su computadora, smartphone o tableta.
Seguro y conforme
pdfFiller le permite gestionar documentos de forma segura cumpliendo con leyes globales como ESIGN, CCPA y GDPR. También cumple con HIPAA y SOC 2.
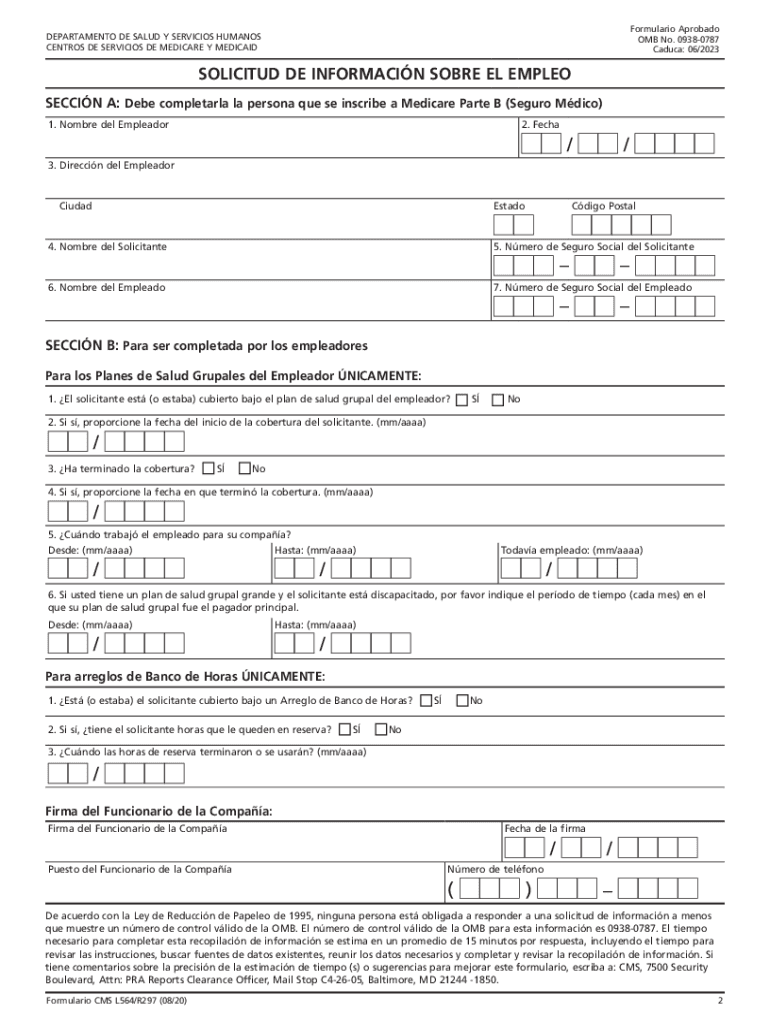
¿Qué es CMS-L564 S?
The Medicare Employment Information Request Form is a Medicare enrollment document used by applicants and employers to verify group health coverage for Medicare Part B enrollment.
pdfFiller obtiene las mejores calificaciones en plataformas de reseñas
¿Quién necesita CMS-L564 S?
Descubre cómo profesionales de distintos sectores usan pdfFiller.

CMS-L564 S es necesario para:
-
Individuals applying for Medicare Part B benefits
-
Employers providing health insurance to employees
-
Social Security Administration staff reviewing Medicare applications
-
Healthcare providers verifying insurance status
-
Insurance agents assisting clients with Medicare enrollment
Guía completa de CMS-L564 S
Understanding the Medicare Employment Information Request Form (CMS L564)
The Medicare Employment Information Request Form, known as the CMS L564, is essential for those enrolling in Medicare. This document verifies group health coverage, which is a prerequisite for Medicare Part B enrollment. Both the applicant and the employer must provide information and signatures on the form to confirm eligibility and health insurance status.
This form plays a crucial role in the enrollment process, ensuring that applicants can smoothly transition to Medicare by validating their existing group health coverage.
Who Should Complete the CMS L564 Form?
Understanding who needs to complete the CMS L564 form is vital for a successful Medicare enrollment. Individuals eligible to apply for Medicare must fill out the form alongside their employers, who also have specific responsibilities in this process. For those transitioning to Medicare, accurately completing this form is critical to secure their health insurance coverage.
Applicants must gather necessary information from their employers to ensure a seamless completion of the CMS L564 form.
Benefits of Using the CMS L564 Form
Using the CMS L564 form offers several advantages in the Medicare enrollment journey. Primarily, it simplifies the verification process of group health coverage, which is essential for enrollment in Medicare Part B. Timely completion of this form can significantly reduce potential delays, allowing for a smoother transition into Medicare.
Additionally, the form minimizes complexities associated with the enrollment process, ensuring that applicants can focus on their health needs without unnecessary setbacks.
How to Fill Out the CMS L564 Form Online: A Step-by-Step Guide
To successfully complete the CMS L564 form online, follow these steps:
-
Access the CMS L564 form through the appropriate online platform.
-
Fill out the applicant’s section, providing personal details like name and Medicare number.
-
Provide the employer's information, including the company name and coverage dates.
-
Ensure both parties sign the form to validate the submission.
-
Review all entries to confirm accuracy before finalizing the submission.
Verification of information is essential to avoid processing issues that could delay Medicare enrollment.
Common Errors and How to Avoid Them When Completing the CMS L564
Several common errors can lead to rejections of the CMS L564 form. Frequent mistakes include:
-
Incomplete personal information from either the applicant or the employer.
-
Omitting required signatures, which can stall the process.
-
Inaccurate health coverage dates, leading to confusion during verification.
To avoid such errors, carefully review the completed form and ensure all information is up-to-date and accurate before submission. Taking the time to double-check can save applicants from unnecessary delays.
Submission Guidelines for the CMS L564 Form
When it comes to submitting the CMS L564 form, there are several methods available:
-
In-person delivery to your local Social Security office.
-
Mail submission, ensuring you account for processing times.
-
E-filing through authorized online platforms, where available.
Be aware of the deadlines for filing the form to avoid late enrollment penalties. Keeping a copy of the submitted form is vital for personal records and future reference.
What Happens After Submitting the CMS L564 Form?
After submission, applicants can expect the following steps in the Medicare enrollment process:
-
The form undergoes processing, with typical timelines varying depending on local office workloads.
-
Applicants can check the status of their submission through the Social Security Administration's tools.
-
If the form is rejected, there may be specific corrective actions required to address the issues.
Understanding these steps prepares applicants for what to expect, allowing them to stay informed throughout the process.
Security and Compliance in Handling the CMS L564 Form
Data safety is paramount when handling the CMS L564 form. Ensuring the protection of sensitive information during submission involves several best practices:
-
Using secure platforms with encryption to transmit information safely.
-
Adhering to compliance standards such as HIPAA and GDPR to protect user data.
-
Utilizing digital tools that offer secure document handling features.
With the right precautions, applicants can submit their forms confidently, knowing their personal information is protected.
Leveraging pdfFiller for Your CMS L564 Form Needs
pdfFiller offers an intuitive solution for filling out and submitting the CMS L564 form efficiently. With user-friendly features designed for ease of use, applicants can quickly edit, complete, and eSign their forms. Enhanced security measures help protect user data throughout the process.
The platform simplifies form filling and improves overall efficiency, making it an excellent choice for those navigating the Medicare enrollment process.
Cómo completar el formulario CMS-L564 S
-
1.To start, access the Medicare Employment Information Request Form on pdfFiller by searching for the form name or using a direct link.
-
2.Once the form is open, familiarize yourself with the layout and available fields.
-
3.Gather required information such as your personal details, your employer’s information, and health coverage details.
-
4.Begin filling out the applicant section by entering your name, address, Social Security number, and coverage dates.
-
5.Navigate to the employer section and input the employer's name, address, and contact information, ensuring accuracy.
-
6.Complete the coverage verification fields by checking the appropriate boxes regarding your health insurance status.
-
7.Once all fields are completed, carefully review the entries for accuracy and completeness.
-
8.After reviewing, ensure both you and your employer have signed the form in the designated areas.
-
9.To save your progress, click the save button and choose a file format like PDF or Word.
-
10.Finally, you can download the filled form or choose to submit it directly via pdfFiller to the local Social Security office.

Preguntas frecuentes
Si no encuentras lo que buscas, ¡contáctanos en cualquier momento!
What are the eligibility requirements for using this form?
To use the Medicare Employment Information Request Form, you must be eligible for Medicare and have group health coverage through your employer or a family member's employer.
Is there a deadline for submitting this form?
While there is no strict deadline for submission, it is recommended to submit the form as soon as possible to avoid delays in Medicare Part B enrollment and coverage.
How do I submit the completed form?
You can submit the completed Medicare Employment Information Request Form either by mailing it to your local Social Security office or digitally submitting it through pdfFiller if available.
What supporting documents are required with this form?
Typically, you should include proof of your health coverage, such as insurance cards or policy documents, along with the completed Medicare Employment Information Request Form.
What common mistakes should I avoid when filling out this form?
Common mistakes include entering incorrect personal information, failing to secure both signatures, and overlooking required fields. Double-check each section before submitting.
How long does it take to process the form?
Processing times can vary, but generally, it may take several weeks for the Social Security Administration to review and process your enrollment request.
What if I have questions while filling out the form?
If you have questions, consider reaching out to your employer for assistance, contacting the Social Security Administration, or checking online resources about Medicare enrollment.
CMS-L564 S Form Versions
Formularios relacionados




Si crees que esta página debe ser retirada, sigue nuestro proceso de retirada DMCA
aquí
.
Este formulario puede incluir campos para información de pago. Los datos introducidos en estos campos no están cubiertos por el cumplimiento de PCI DSS.